Understanding MG: Beyond Acetylcholine Receptor Antibodies — The Overlooked Pathogenic Mechanisms and Research Hotspots
Imagine waking up full of energy in the morning, only to experience drooping eyelids, slurred speech, and barely enough strength to hold chopsticks by the afternoon. This is the daily reality for patients with myasthenia gravis. Myasthenia gravis (MG) is an autoimmune neuromuscular disorder characterized by fatigable muscle weakness, primarily disrupting signal transmission at the neuromuscular junction (NMJ). Symptoms typically fluctuate and often begin with ocular muscles (e.g., ptosis, diplopia), potentially spreading to facial, bulbar, limb, and respiratory muscles.
The incidence of MG is approximately 5–30 cases per million people annually, with a higher prevalence in women (especially ages 20–40) and older men. About 80–90% of patients have detectable autoantibodies against the acetylcholine receptor (AChR) in their serum, while other subtypes involve antibodies to muscle-specific kinase (MuSK) or low-density lipoprotein receptor-related protein 4 (LRP4). MG is often associated with thymoma, and thymic abnormalities are common in AChR-positive patients.
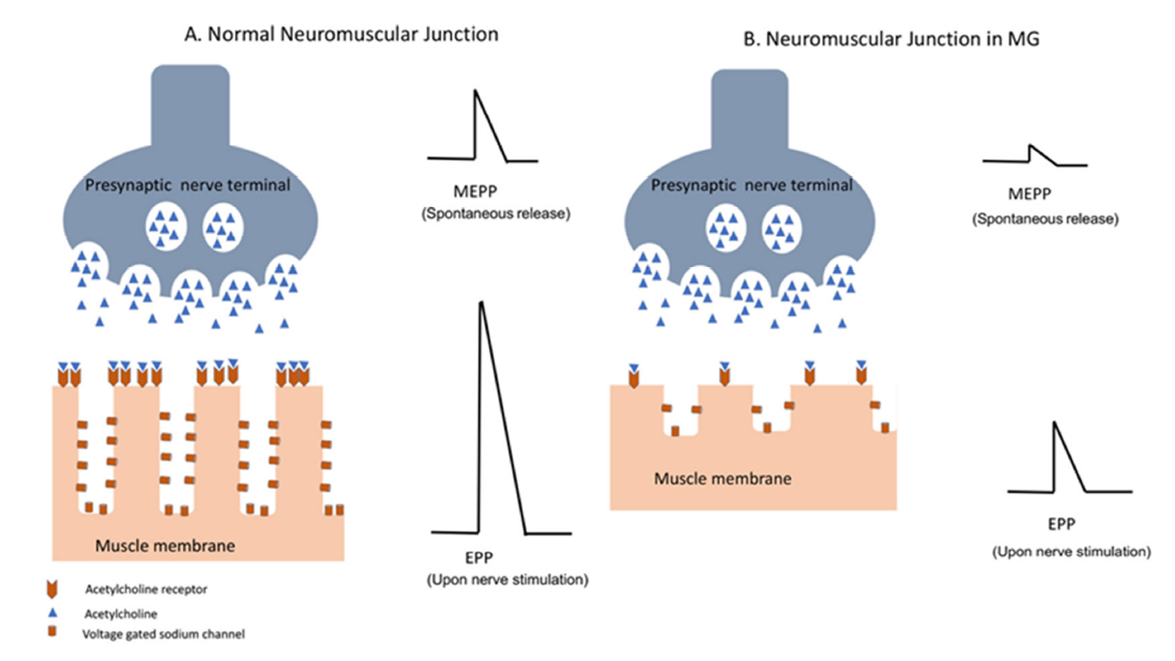
Figure 1. Neuromuscular transmission in a healthy individual (A) and a patient with myasthenia gravis (B)
Clinically, MG is classified as ocular (limited to the eyes) or generalized (affecting multiple muscle groups). In severe cases, it can lead to respiratory failure (myasthenic crisis). Diagnosis relies on clinical symptoms, serum antibody testing, repetitive nerve stimulation, and single-fiber electromyography. Prognosis is generally favorable with long-term symptom management.
Pathogenic Mechanisms
The core pathology of MG is autoimmune-mediated NMJ dysfunction. Pathogenic autoantibodies target key proteins on the postsynaptic membrane, impairing acetylcholine (ACh) signaling. Key details include:
- AChR-positive MG (most common, ~80%): IgG1/IgG3 antibodies bind AChR, triggering complement activation, membrane attack complex (MAC) formation, AChR internalization and degradation (antigenic modulation), and direct blockade of ACh binding — ultimately reducing AChR density and muscle excitability.
- MuSK-positive MG (~5–10%): IgG4 antibodies inhibit MuSK phosphorylation, disrupting the LRP4-agrin complex and impairing AChR clustering and NMJ stability.
- LRP4-positive MG: IgG1 antibodies interfere with LRP4-agrin binding, indirectly suppressing MuSK activation while also activating complement.
- Thymic involvement: AChR-positive MG is frequently linked to thymic hyperplasia or thymoma, where aberrant B cells in the thymus produce autoantibodies and T cells contribute to loss of immune tolerance.
- Genetic and environmental factors: HLA-associated susceptibility genes; triggers may include infections or medications.
These processes damage the postsynaptic membrane, reduce the safety factor, and worsen fatigability with repeated muscle use.
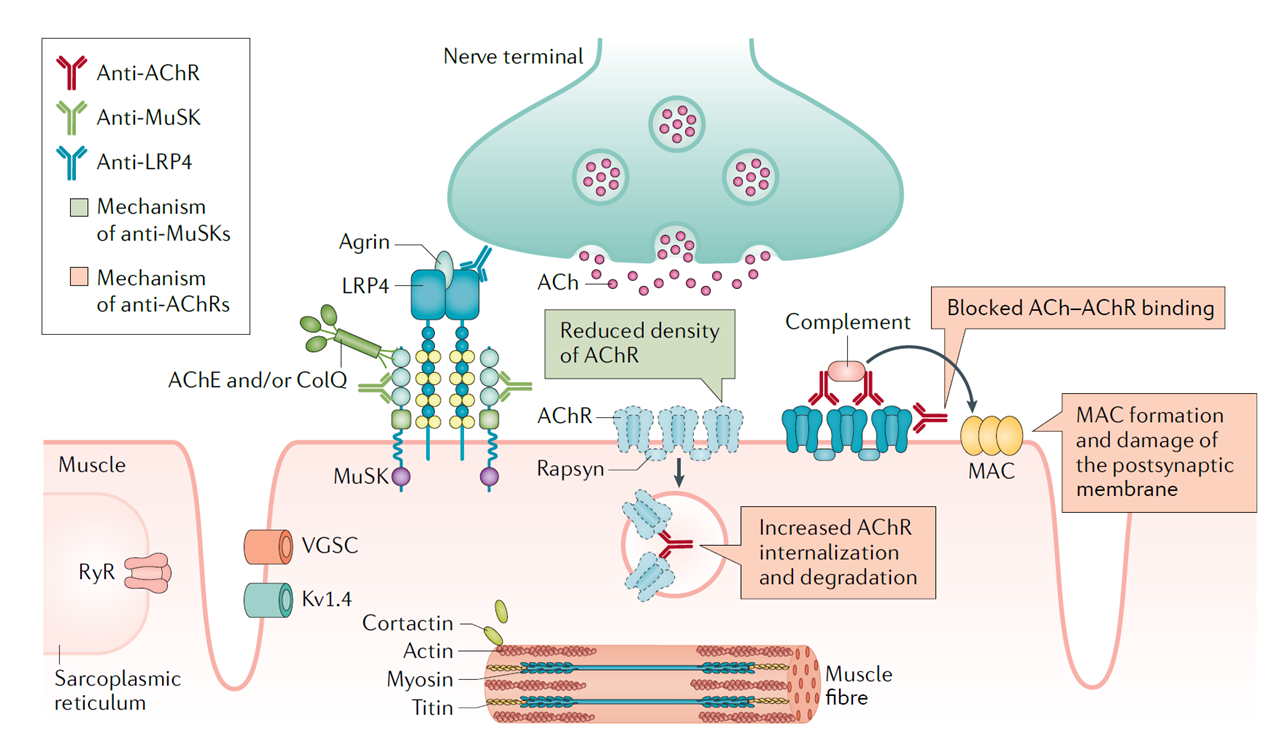
Figure 2. Pathophysiology of MG at the neuromuscular junction
Key Frontier Advances and Targets
1. Terminal Complement Pathway Inhibition (C5 Inhibition)
Mechanism: AChR antibodies (primarily IgG1/IgG3) activate the classical complement pathway, cleaving C5 to form the MAC, which damages postsynaptic folds and AChRs. C5 inhibitors block C5 cleavage, prevent MAC assembly, and protect the NMJ without affecting upstream complement functions.
Key approved agents (based on Phase III data):
- Eculizumab (Soliris): First approved (2017); REGAIN trial showed significant improvements in MG-ADL and QMG scores.
- Ravulizumab (Ultomiris): Long-acting C5 mAb administered IV every 8 weeks; CHAMPION MG trial confirmed sustained efficacy (MG-ADL improvement at 26 weeks) and good safety.
- Zilucoplan (Zilbrysq): Small-molecule peptide C5 inhibitor for daily subcutaneous self-injection; RAISE Phase III and RAISE-XT open-label extension (up to 96 weeks) demonstrated ongoing MG-ADL improvement with high tolerability and convenience.
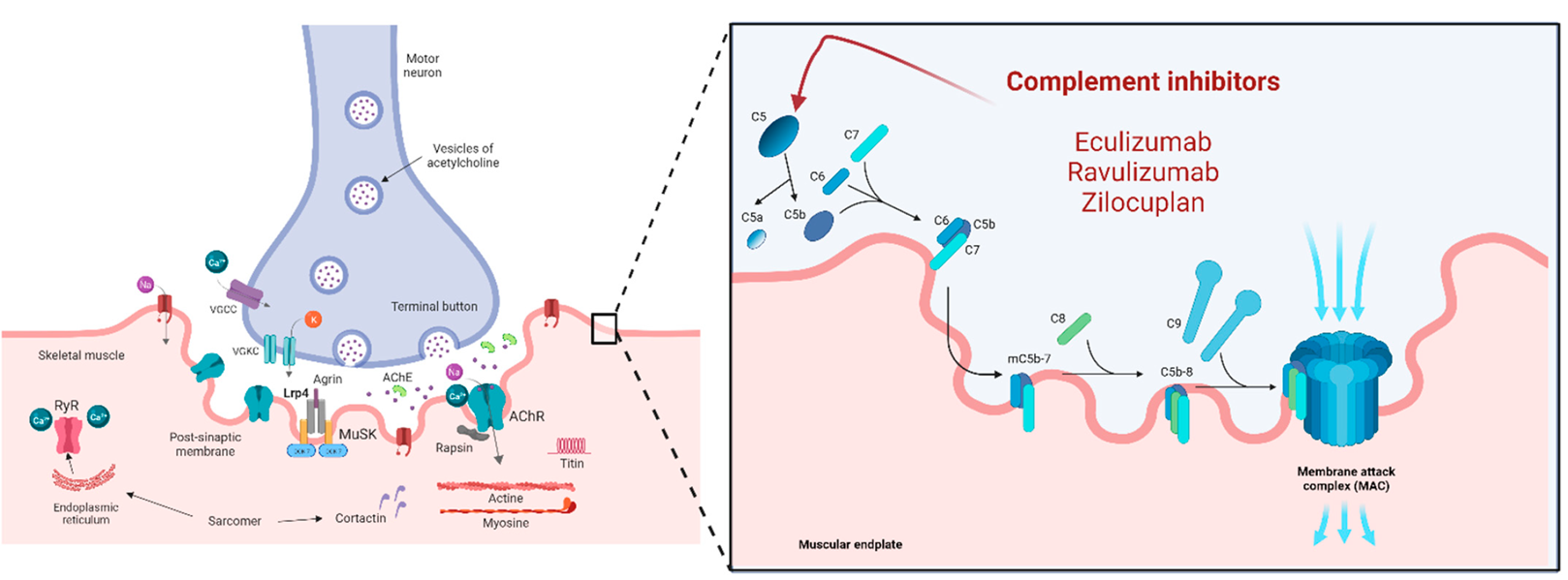
Figure 3. Complement inhibitors and their mechanisms of action
2. Neonatal Fc Receptor (FcRn) Blockade
Mechanism: FcRn binds IgG in acidic endosomes, preventing lysosomal degradation and recycling it — prolonging the half-life of pathogenic IgG (including AChR/MuSK antibodies). FcRn inhibitors competitively block IgG-FcRn binding, accelerating IgG catabolism and rapidly reducing circulating IgG levels (typically by 60–80%), thereby decreasing NMJ damage.
Key agents:
- Efgartigimod (Vyvgart / Vyvgart Hytrulo): IV or subcutaneous; ADAPT series showed rapid onset (cyclic dosing, significant MG-ADL improvement); 2025 ADAPT extensions confirmed efficacy in MuSK+, LRP4+, and triple-negative cases.
- Rozanolixizumab (Rystiggo): Weekly subcutaneous; MycarinG and open-label extensions showed notable improvement in ocular symptoms; 2025 EU approval for self-administration enhances convenience.
- Nipocalimab (Imaavy): FDA approved April 2025; Vivacity-MG3 and OLE demonstrated sustained QMG/MG-ADL control across AChR+/MuSK+/LRP4+ subtypes.
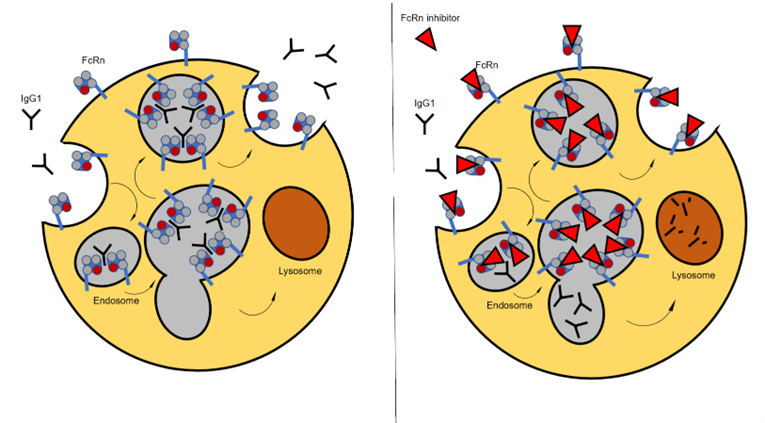
Figure 4. Mechanism of FcRn-targeted therapies
3. B-Cell Targeting and Other Emerging Therapies
Rituximab (anti-CD20 mAb): Depletes CD20+ B cells; most effective in MuSK+ MG (often achieving long-term remission), with partial benefit in AChR+ cases.
Inebilizumab (anti-CD19 mAb): FDA approved December 2025 based on Phase 3 MINT trial (NEJM 2025); long-acting (twice yearly after loading doses), targets a broader B-cell population including plasmablasts.
CAR-T cell therapy (targeting pathogenic plasma/B cells):
- Descartes-08 (mRNA BCMA CAR-T): Phase 2b updates showed deep, durable responses (significant MG-ADL/QMG reductions); Phase 3 AURORA planned for 2025.
- KYV-101 (CD19 CAR-T): KYSA-6 Phase 2 interim data (2025 AANEM) indicated high rates of minimal symptom expression after a single dose, with good tolerability.
- CABA-201 (CD19 CAR-T): RESET-MG Phase 1/2 ongoing, aiming for durable/potentially curative remission.
These emerging therapies shift from nonspecific suppression toward precise elimination of pathogenic B/plasma cells, offering potential for long-term drug-free remission — though risks like infection and cytokine release syndrome require careful monitoring.
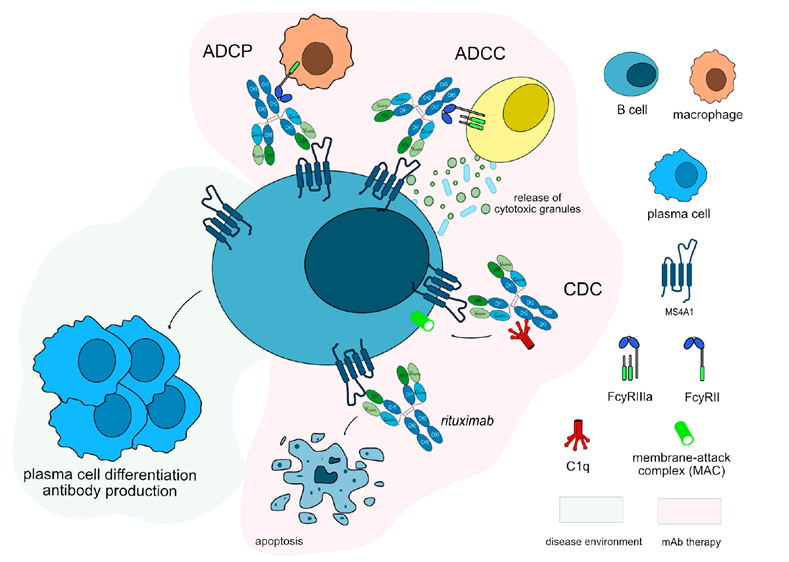
Figure 5. Mechanism of action of Rituximab
abinScience Related Products
The following abinScience products target core pathways in myasthenia gravis research, including NMJ structural proteins (AChR/MuSK/LRP4/Agrin), complement C5, FcRn, and B-cell surface markers (CD20/CD19). Catalog numbers link directly to product pages.
Antibody
| Catalog No. |
Product Name |
| HX061056 |
Research Grade Efgartigimod |
| HX061046 |
Research Grade Nipocalimab |
| HX061026 |
Research Grade Rozanolixizumab |
| HF687026 |
Research Grade Eculizumab |
| HF687016 |
Research Grade Ravulizumab |
| HB996026 |
Research Grade Inebilizumab |
| HY257056 |
Research Grade Rituximab |
| AF687014 |
Anti-Eculizumab Polyclonal Antibody |
| AY257024 |
Anti-Rituximab Polyclonal Antibody |
Protein
| Catalog No. |
Product Name |
| HF829012 |
Recombinant Human CHRNA1 Protein, N-GST |
| HF829022 |
Recombinant Human CHRNA1 Protein, N-His |
| HT224012 |
Recombinant Human MUSK Protein, N-His |
| HF599012 |
Recombinant Human LRP4 Protein, N-GST |
| HT005012 |
Recombinant Human AGRN Protein, N-His |
| HF687012 |
Recombinant Human C5 Protein, N-GST |
| HF687022 |
Recombinant Human C5 Protein, N-His |
| HX061012 |
Recombinant Human FCGRT Protein, N-His |
| HY257012 |
Recombinant Human CD20/MS4A1 Protein, N-His |
| HB996012 |
Recombinant Human CD19 Protein, N-His |
| HF829032 |
Recombinant Human CHRNA1 Protein, C-His |
| HV212012 |
Recombinant Human CD257/BAFF/TNFSF13B Protein, N-His |
| HV212011 |
Recombinant Human CD257/BAFF/TNFSF13B Protein, N-Fc |
| HV212021 |
Recombinant Human CD257/BAFF/TNFSF13B Protein, C-His |
| HY328012 |
Recombinant Human IL6 Protein, N-His |
| HB990012 |
Recombinant Human CD119/IFNGR1 Protein, N-His |
| HF974012 |
Recombinant Human HLA-DRB1 Protein, N-His |
View more Protein products
Kit
| Catalog No. |
Product Name |
| AF687028 |
Anti-Eculizumab Neutralizing Antibody ELISA Kit |
| AF687018 |
Anti-Eculizumab ELISA Kit |
| DF687028 |
Eculizumab ELISA Kit |
| AY257018 |
Anti-Rituximab ELISA Kit |
Looking for Myasthenia Gravis Research Tools?
abinScience provides factory-direct recombinant proteins and antibodies for AChR, MuSK, LRP4, C5, FcRn, and B-cell targets — with bulk pricing, custom specifications, and technical consultation available.
Email: info@abinscience.com | Tel: +86-27-65523339
References:
1. Gilhus NE, Tzartos S, Evoli A, et al. Myasthenia gravis. Nat Rev Dis Primers. 2019;5(1):30. doi: 10.1038/s41572-019-0079-y
2. Howard JF Jr, Utsugisawa K, Benatar M, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3 randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol. 2017;16(12):976-986. doi: 10.1016/S1474-4422(17)30369-1
3. Vu T, Meisel A, Bhatt P, et al. CHAMPION MG: Phase 3 results of ravulizumab in generalized myasthenia gravis. Neurology. 2024;102(12):e209367. doi: 10.1212/WNL.0000000000209367
4. Howard JF Jr, Bril V, Vu T, et al. Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021;20(7):526-536. doi: 10.1016/S1474-4422(21)00159-9
5. Nowak R, Benatar M, Ciafaloni E, et al. A phase 3 trial of inebilizumab in generalized myasthenia gravis. N Engl J Med. 2025;392(23):2309-2320. doi: 10.1056/NEJMoa2501561
6. Johnson & Johnson. FDA approval of Imaavy (nipocalimab-aahu) for gMG. Press release, April 30, 2025. https://www.jnj.com

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский


