2026 Lung Cancer Research Review: Molecular Targets, Clinical Breakthroughs & Research Reagents
Release date:
2026-04-21 View count: 61
2026 Lung Cancer Research Review: EGFR, ALK, KRAS G12C, PD-L1 — Molecular Targets, Clinical Breakthroughs & Research Reagents
Lung cancer remains the leading cause of cancer-related mortality worldwide, accounting for approximately 2.5 million new cases and 1.8 million deaths annually. Non-small cell lung cancer (NSCLC) constitutes ~85% of all cases, with adenocarcinoma as the predominant histological subtype, while small cell lung cancer (SCLC) accounts for ~15% and is characterized by rapid proliferation, early metastasis, and frequent relapse. The past decade has witnessed a paradigm shift from empirical chemotherapy toward precision oncology driven by actionable genomic alterations. Today, comprehensive molecular profiling at diagnosis is the standard of care — identifying driver mutations in EGFR, ALK, KRAS G12C, ROS1, MET, RET, and BRAF V600E, along with PD-L1 expression status, fundamentally determines treatment strategy and patient outcomes.
Actionable Molecular Targets in Lung Cancer
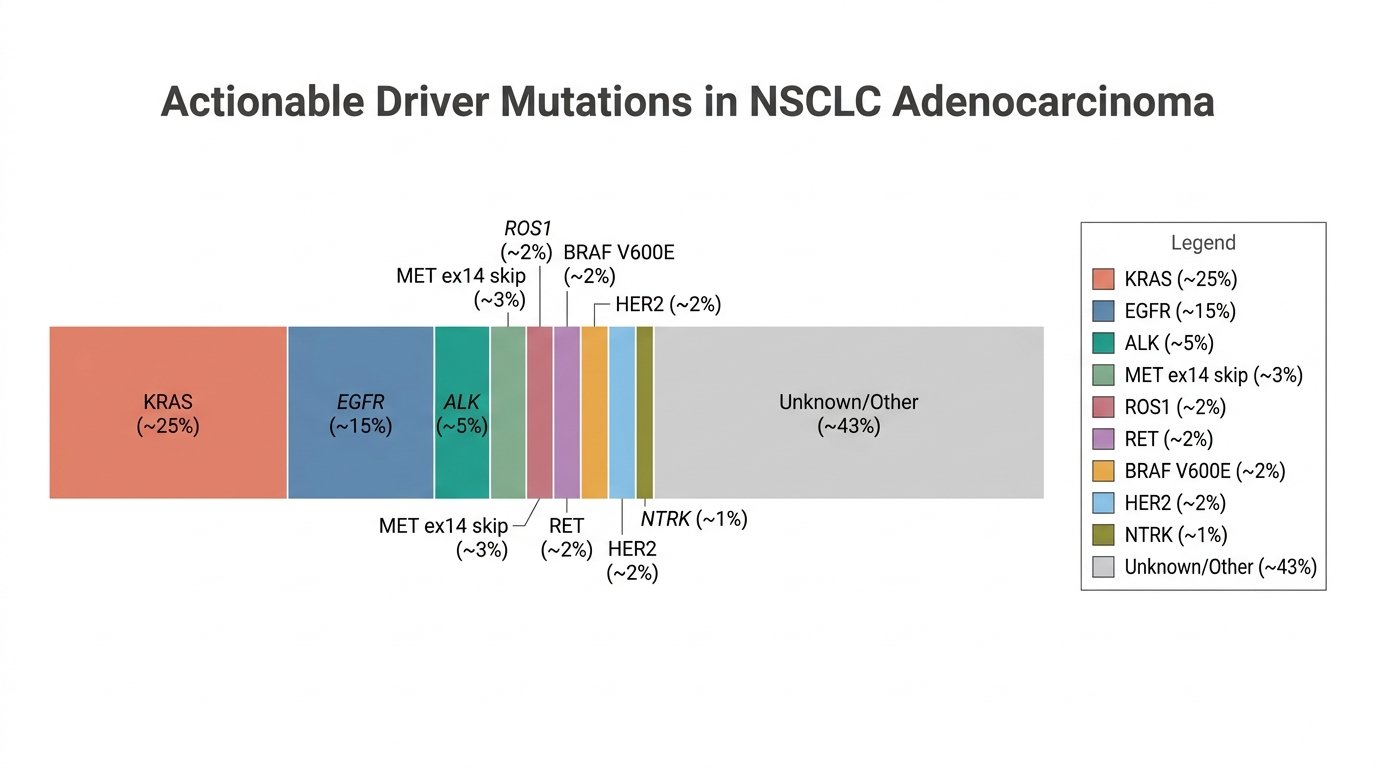
Comprehensive genomic profiling has revealed a complex mutational landscape in NSCLC. The table below summarizes the major clinically actionable targets, their biological roles, prevalence in NSCLC, and the therapeutic strategies currently employed.
Figure 1. Actionable Driver Mutations in NSCLC Adenocarcinoma. KRAS (~25%) and EGFR (~15%) are the most prevalent drivers, followed by ALK (~5%), MET exon 14 skipping (~3%), ROS1, RET, BRAF V600E, and HER2 (each ~2%). Approximately 43% of cases harbor no currently actionable driver.
Target
Biological Function
NSCLC Prevalence
Pathological Role
Approved Therapies (Examples)
EGFR
Receptor tyrosine kinase driving RAS/RAF/MEK/ERK and PI3K/AKT signaling cascades that promote cell proliferation and survival
10–15% (Western); 40–55% (East Asian)
Activating mutations (exon 19 del, L858R, exon 20 ins, T790M) lead to constitutive kinase activation and oncogenic signaling
Osimertinib, Amivantamab, Cetuximab, Erlotinib
ALK
Receptor tyrosine kinase normally involved in nervous system development
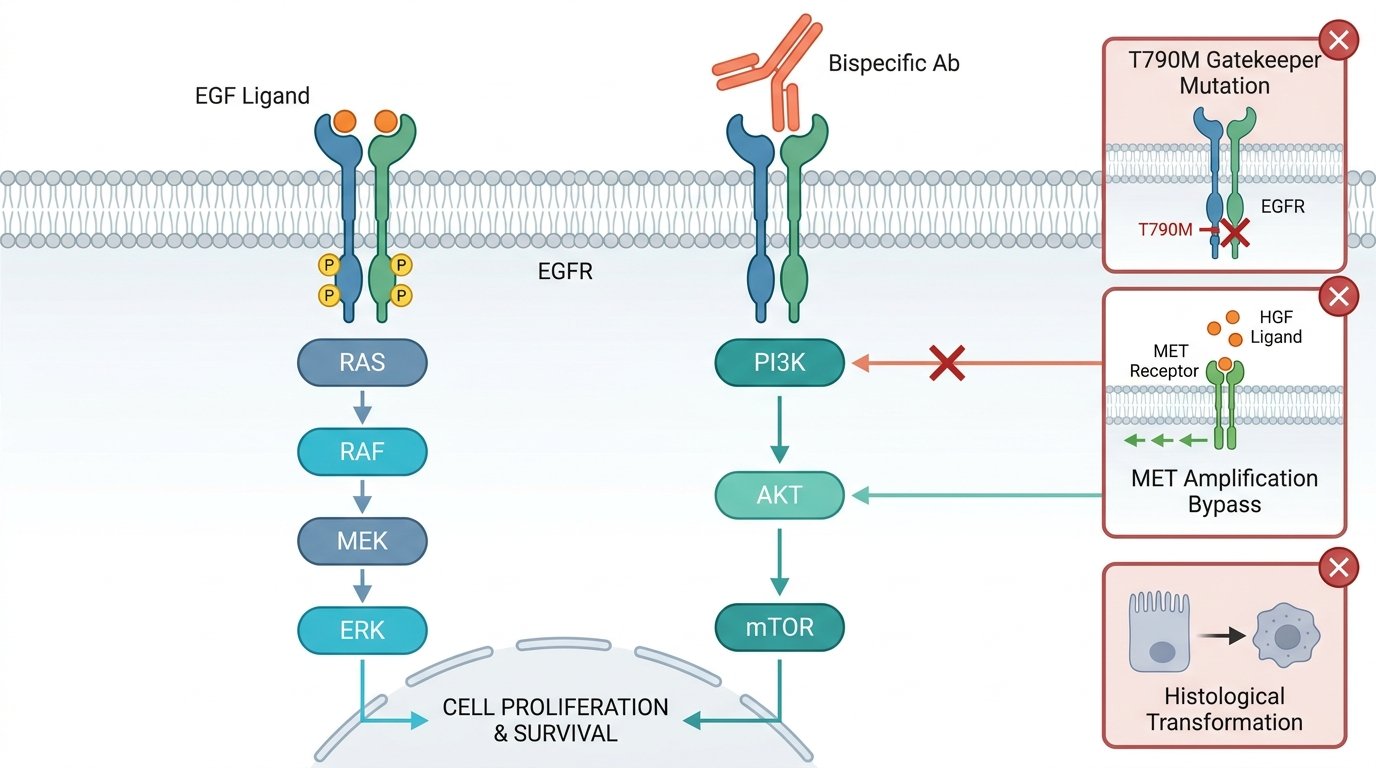
The epidermal growth factor receptor (EGFR/ERBB1/HER1) is a transmembrane receptor tyrosine kinase that, upon EGF ligand binding, undergoes homo- or hetero-dimerization (with ERBB2/HER2, ERBB3/HER3) and autophosphorylation, activating three major downstream cascades: RAS–RAF–MEK–ERK (proliferation), PI3K–AKT–mTOR (survival), and JAK–STAT (transcription). In NSCLC, EGFR-activating mutations are the most common actionable alterations, particularly in East Asian, female, and never-smoker populations.
Figure 2. EGFR Signaling Pathways and Acquired Resistance Mechanisms. Left: EGF-induced receptor dimerization and phosphorylation activate the RAS–RAF–MEK–ERK and PI3K–AKT–mTOR cascades. Right: Bispecific antibody blockade and three major post-TKI resistance mechanisms — T790M mutation, MET amplification bypass, and histological transformation.
Key Mutation Classes and Clinical Significance:
Classical mutations (~85%): Exon 19 deletions and exon 21 L858R point mutations are highly sensitive to first-, second-, and third-generation EGFR TKIs. Third-generation osimertinib (FLAURA study) has become the global first-line standard of care.
Exon 20 insertions (~10%): Historically resistant to conventional TKIs. The EGFR-MET bispecific antibody amivantamab plus chemotherapy (PAPILLON trial, NEJM 2024) achieved median PFS of 11.4 months vs. 6.7 months for chemotherapy alone, establishing a new treatment paradigm for this subset.
T790M gatekeeper mutation: Most common acquired resistance mechanism to first/second-generation TKIs; effectively overcome by osimertinib.
Post-osimertinib resistance (2025 frontier): Mechanisms include C797S mutation, MET amplification, histological transformation to SCLC, and off-target bypass via HER2/HER3 activation. The MARIPOSA trial showed amivantamab + lazertinib improved PFS over osimertinib alone as first-line therapy (23.7 vs. 16.6 months), addressing early resistance prevention.
These findings have expanded the therapeutic landscape from single-target TKIs to bispecific antibodies, antibody-drug conjugates (ADCs), and combination strategies, making EGFR pathway reagents essential tools for mechanistic research and drug development.
Current Clinical Reality: Molecular testing for EGFR, ALK, KRAS G12C, ROS1, MET, RET, BRAF, PD-L1, and NTRK is now recommended by NCCN guidelines for all patients with advanced NSCLC at diagnosis. Treatment decisions are fundamentally driven by genomic profiling results.
Lung Cancer Latest Research & Clinical Progress (2024–2026)
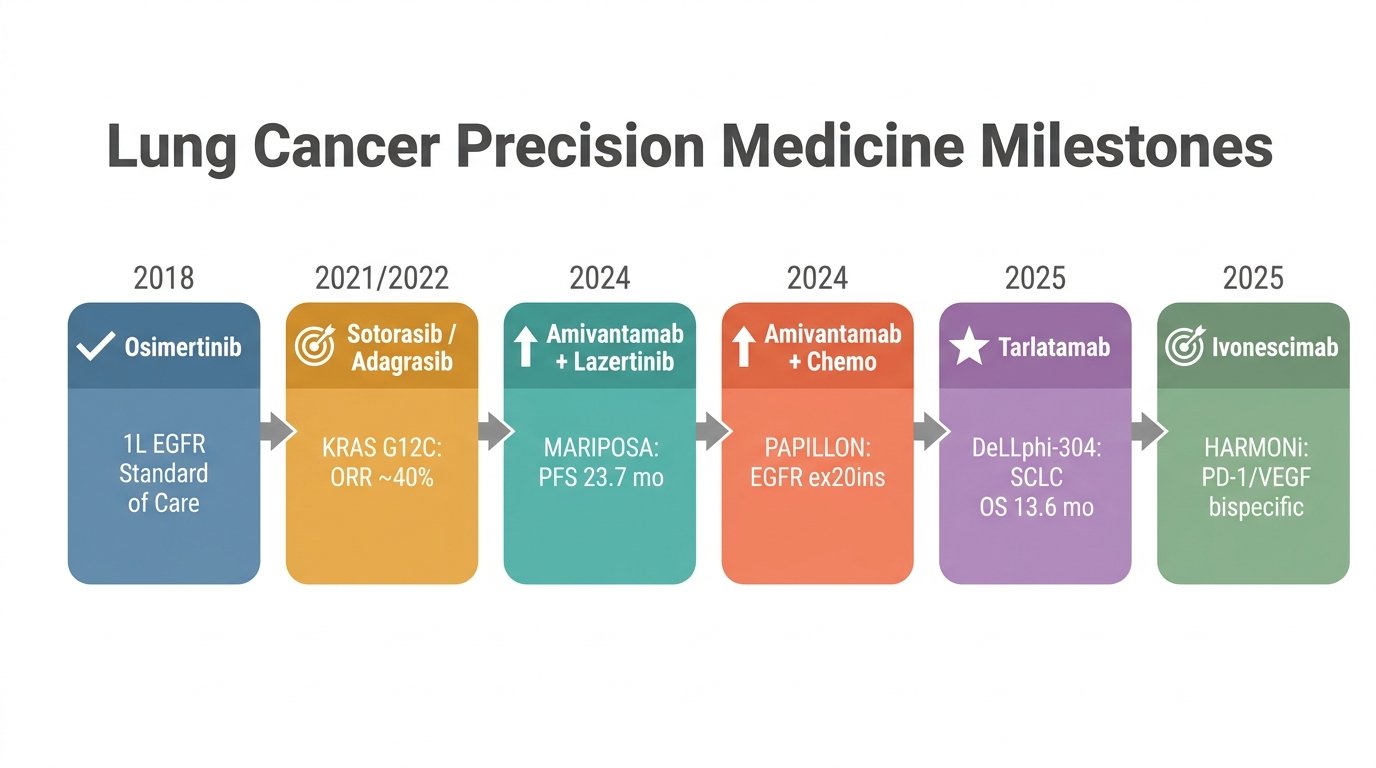
Figure 3. Lung Cancer Precision Medicine Milestones (2018–2025). Chronological overview of landmark therapeutic advances: osimertinib as first-line EGFR standard of care, KRAS G12C inhibitors (sotorasib/adagrasib), EGFR–MET bispecific combinations (MARIPOSA & PAPILLON), DLL3-targeted tarlatamab in SCLC, and PD-1/VEGF bispecific ivonescimab.
Median PFS 11.4 vs. 6.7 months (HR 0.40); ORR 73% vs. 47%. First bispecific antibody regimen to show superiority over chemotherapy in EGFR ex20ins NSCLC.
Establishes amivantamab + carboplatin–pemetrexed as the new first-line standard for EGFR exon 20 insertion NSCLC.
PFS 23.7 vs. 16.6 months over osimertinib alone (HR 0.70). First regimen to significantly improve PFS beyond osimertinib in first-line EGFR-mutant NSCLC.
Challenges osimertinib monotherapy dominance; highlights the benefit of dual EGFR + MET blockade with concurrent TKI therapy.
—
Tarlatamab (DLL3 BiTE; DeLLphi-304 Phase 3, SCLC)
Median OS 13.6 vs. 8.3 months (HR 0.60; P<0.001) vs. chemotherapy in relapsed SCLC; 40% reduction in risk of death.
First targeted immunotherapy to demonstrate OS benefit in second-line SCLC. DLL3-targeted BiTE represents a paradigm shift from chemotherapy in relapsed SCLC.
PFS HR 0.51 vs. pembrolizumab monotherapy in PD-L1–positive NSCLC; consistent benefit across squamous and non-squamous histologies. HARMONi-3 (vs. pembro + chemo) ongoing.
First PD-1/VEGF bispecific to outperform pembrolizumab; dual checkpoint/anti-angiogenic blockade in a single molecule may redefine first-line I/O in NSCLC.
—
Sotorasib & Adagrasib (KRAS G12C inhibitors)
Both FDA-approved for previously treated KRAS G12C NSCLC; ORR ~36–43%, mPFS ~5.6–6.5 months. Combination strategies (sotorasib + chemo, SCARLET: ORR 89%) and next-gen pan-KRAS inhibitors (RMC-6236) actively in trials.
Landmark “undruggable” target breakthrough; monotherapy benefit is limited, driving intensive combination and next-gen inhibitor development.
[2]
Zipalertinib (EGFR ex20ins oral TKI)
ORR 35% overall; 40% in amivantamab-naive patients. Oral administration provides a convenient alternative to IV-based amivantamab.
Expands treatment options for EGFR exon 20 insertion NSCLC with an oral-first approach; activity retained post-amivantamab (ORR 30%).
—
R&D Trends: Bispecific antibodies (amivantamab, ivonescimab, tarlatamab) represent the most rapidly advancing therapeutic class in lung cancer. Combination strategies — bispecific + TKI, bispecific + chemotherapy, and dual immune checkpoint blockade — are reshaping treatment algorithms. Research-grade biosimilars of these agents are essential for preclinical validation, PK/ADA assay development, and mechanism-of-action studies.
abinScience Lung Cancer Research Reagents
abinScience offers a comprehensive portfolio of 800+ products covering all major lung cancer targets — recombinant proteins, research-grade antibodies (polyclonal, monoclonal, nanobody), biosimilar reference standards, InVivoMAb functional antibodies, ELISA kits, and stable cell lines. Below is a curated selection of representative products organized by target and product type.
abinScience — Empowering Bioscience Discovery From EGFR pathway antibodies and KRAS G12C mutant proteins to PD-1/PD-L1 checkpoint biosimilars and ELISA kits, abinScience provides a complete toolkit for lung cancer target validation, drug screening, PK/ADA assay development, and biomarker research. Explore the full catalog of 800+ lung cancer reagents.
Zhou C, Tang KJ, Cho BC, et al. Amivantamab plus chemotherapy in NSCLC with EGFR exon 20 insertions. N Engl J Med. 2023;389(22):2039–2051. doi:10.1056/NEJMoa2306441
Skoulidis F, Li BT, Dy GK, et al. Sotorasib for lung cancers with KRAS p.G12C mutation. N Engl J Med. 2021;384(25):2371–2381. doi:10.1056/NEJMoa2103695
Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446–454. doi:10.1038/nature25183

 中文
中文 English
English 한국어
한국어 日本語
日本語 Español
Español Français
Français Русский
Русский